Case 1.
A 67-year-old patient from Melbourne presented with severe back pain rated 8/10 after failed physiotherapy, SIJ prolotherapy, and pain management.
- SIJ injection gave only 24 hours of relief, but that response remained diagnostically important.
- Beighton score: 7/9.
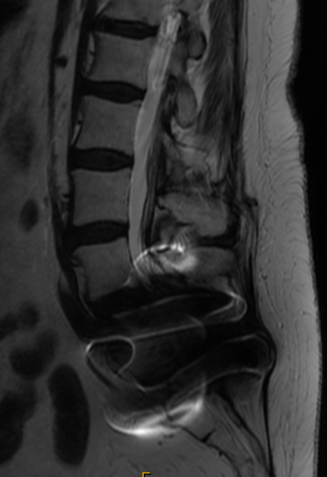
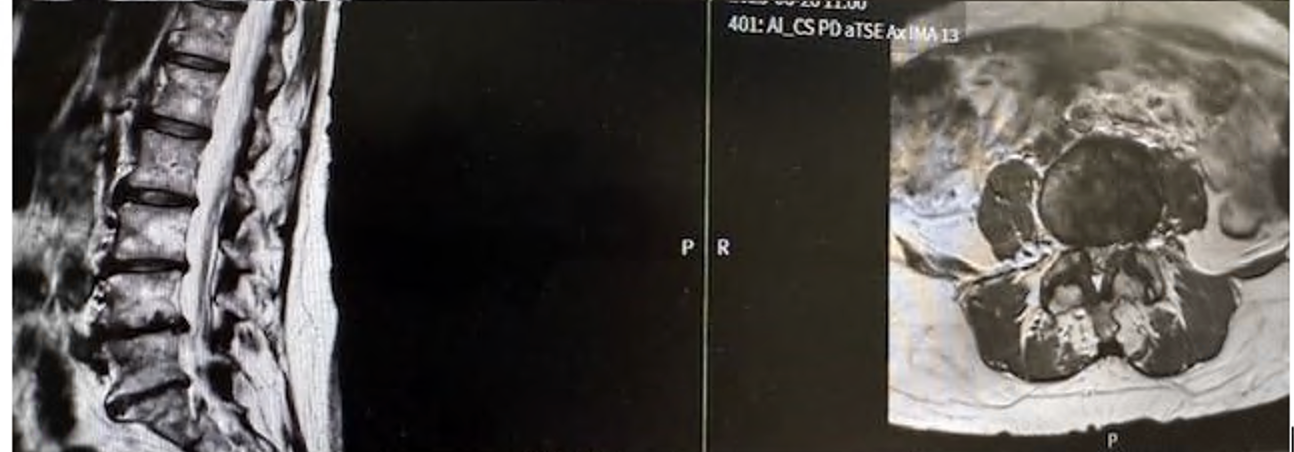
- MRI showed severe discovertebral degeneration and facet arthritis.